
COVID DEATHS COMPARED: US AND INDIA
COVID DEATHS COMPARED: US AND INDIA
Even accounting for under-counts in India, the burden of death in the United States is not that much different

COVID DEATHS COMPARED: US AND INDIA
29 May 2021/Saturday/1000am PDT
"We long to return to normal, but **normal led to this**. To avert the future pandemics we know are coming, we MUST grapple with all the ways normal failed us. We have to build something better."
-Science journalist Ed Yong, from his August 2020 article "How the Pandemic Defeated America"
High resolution version of today's pandemic graphic: https://drive.google.com/file/d/1_JCtoa_Q7LtJpkEIxBzW6Xqkkf9-djkc/view?usp=sharing
BACKGROUND
Two common fallacies I see repeatedly in this pandemic are not making proper comparisons of two data points and the idea that "It can't happen here", that somehow prosperity offers material advantages against COVID. And those two fallacies still drive a lot of false narratives on social media and beyond even to this day.
Nowhere have I seen this more in comparisons of the COVID surge in India and the surges we have had here in the United States.
In relation to the first point, I often see people pointing to the high daily COVID death numbers in India as being much higher than our worst days during the holiday surge here in the United States. But what's missed is that from a population standpoint, India is four times the size of the United States. India has a population of 1.33 billion and the United States has a population of 333 million. There are single provinces in India that have a population that are 1/3 the population of the entire United States.
Even news reports in my own home of Dallas/Fort Worth would say something like "1000 new cases in Dallas County" today and it sounds more alarming than it is when you factor in there's 2.6 million residents in Dallas County.
I have mentioned before in the past a more accurate comparison is to normalize for population and one of my preferred parameters for data comparison is to determine the number per 100,000 people. It could be cases per 100,000 people, it could be deaths per 100,000 people, or anything we want to compare using a "standard yardstick". Normalizing for population helps when comparing two locations of differing population size- you can't use absolute numbers of deaths or cases or whatever else. You have to adjust for the population differences.
Looking at case or death data per 100K people gives you an idea of the community burden of the pandemic.
WHAT ARE THE ABSOLUTE NUMBERS FOR THE UNITED STATES AND INDIA?
Let's just look at COVID deaths for now:
India cumulative COVID death toll: 323,000
India worst daily COVID death toll: 18 May 2021, 4539 deaths
India worst 7-day average: 23 May 2021, 4454 deaths
United States cumulative COVID death toll: 594,000
United States worst daily COVID death toll: 12 January 2021, 4475 deaths
United States worst 7-day average: 14 January 2021, 3998 deaths
COMPARISON OF DEATHS NORMALIZED BY POPULATION (7-DAY AVERAGES)
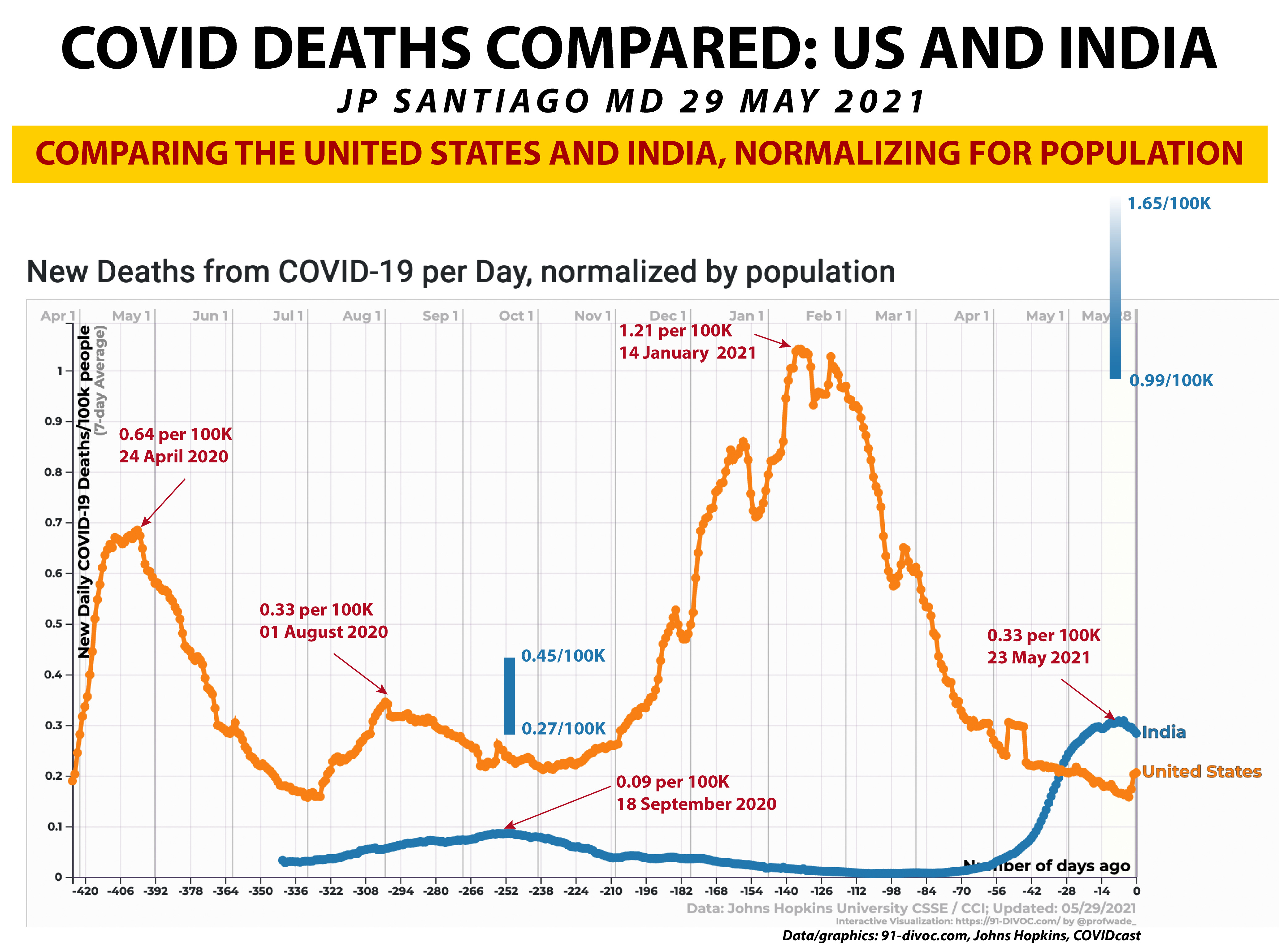
I pulled this graph from 91-divoc.com that uses the Johns Hopkins data set- this tracks daily deaths per 100,000 people since April 1- the United States is the orange line and India is the blue line. I have marked out each of the three peak COVID death surges in the United States and the per 100K number at each point. I have done the same for the two COVID death surges in India as well.
On the surface of it, it was actually quite a bit worse here in the United States than India when looking at the deaths per 100K. But it's been widely reported that COVID deaths in India are significantly under-reported. Many news accounts have looked at the numbers of dead processed in the crematoriums in India. We have all seen the sobering images of multiple funeral pyres all over India.
I highly suggest this Reuters news graphic to understand the scope of the tragedy in India: https://graphics.reuters.com/HEALTH-INDIA/CORONAVIRUS-DEATHS/qzjvqrqaqpx/index.html
Based on crematorium data, estimates range anywhere from the actual COVID death toll in India being 3 to as much as 5 times the official numbers.
On the graph, I have two vertical blue bars that show the possible range of actual COVID deaths based on crematorium data. But what is important to understand here goes to addressing the second fallacy I see in this pandemic- "It can't happen to me/us".
Even if we were to use the vertical blue bars which are based off estimates from cremations done in India, you can see that our three surges here in the United States are STILL very significant and not all that different from the extent of tragedy in India.
Some paint the pandemic environment in India as the product of its caste system, extent of poverty or "poor medical infrastructure"- the data shows the pandemic death toll was just as tragic here in America despite all the self-perceived advantages of our society. Or maybe we do have an unspoken caste system in our society, we have much more poverty than we admit and our medical infrastructure isn't as good as we think.
To the first point, many you know I left private practice to join the Indian Health Service. I have spent a lot of time with an impoverished and marginalized patient population that I can't help but think an unspoken caste system exists here. To the second point about the true extent of our poverty, I should note that the number one reason for personal bankruptcy in the United States are medical costs. A friend of mine once remarked "the average American is one set of tires away from personal bankruptcy". And to my third observation- our medical system is heavily biased to those who have the means and access to get good health care. I saw in private practice with the kinds of insurance plans people had. Some plans were very difficult to work with, others were not. And that distinction is magnified when you spend time practicing medicine with a population like Native Americans or any other group that are made up predominantly of the poor, hourly workers with no wage protections and the marginalized.
TAKE HOME MESSAGES
1/ Always always ALWAYS look at incidents per 100,000 people when comparing the pandemic environment of two or more locations. It gives a more accurate picture of the pandemic burden in a community.
2/ This virus doesn't give a shit if you live in an industrialized superpower or a developing nation.
3/ One of the best things we can do to prepare for the next pandemic is not to return to business as usual but to make a concerted effort at the national, social, political and individual level to build better social, economic and political structures to address inequity and privilege.
PARTING THOUGHTS
Depending upon where you sit in society, the pandemic experience is different. There are those who act to divide us for their own gain but keep in mind there are three kinds of empathy, each of which we need to build a better post-pandemic environment:
Cognitive empathy: The ability to see the world from someone else's perspective.
Emotional empathy: The ability to feel someone else's emotions. This is the first one we experience as children.
Compassionate empathy: The ability to feel concern for someone else and be moved to action.
The real challenge is to have the three types of empathy in relation to someone not like you but different from you. It's easy to have empathy for those who are like us. To have empathy for those different from us is what we are all called to do regardless of your spiritual and moral traditions.
RELEVANT PAST POSTS (PUBLIC FACEBOOK LINKS)
THE B.1.617 FAMILY OF COVID VARIANTS (15 May 2021): https://www.facebook.com/jp.j.santiago/posts/10218856000568009
THE MOLECULAR BIOLOGY OF THE E484K MUTATION (10 May 2021): https://www.facebook.com/jp.j.santiago/posts/10218832046529173
IMMUNOLOGY 101: THE IMMUNE SYSTEM- REPOST/UPDATE (05 May 2021): https://www.facebook.com/jp.j.santiago/posts/10218801066954703
QUICK UPDATE: AMERICAN INDIANS/ALASKA NATIVES LEAD THE WAY ON VACCINATIONS (29 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218763919866049
QUICK UPDATE: BY THE NUMBERS (27 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218750780817581
COVID VARIANTS OVERVIEW AND UPDATE (22 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218722676514991
NEW COVID VARIANT OF INTEREST: B.1.617 (18 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218699298170547
CASE SURGES CAN RESULT IN COVID VARIANTS (12 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218657527966318
THE OVERVIEW & STATUS OF COVID VARIANTS (9 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218637120816152
MAYO CLINIC GRAND ROUNDS: COVID TESTING (12 March 2021): https://www.facebook.com/jp.j.santiago/posts/10218453381862793
QUICK UPDATE: THE COVID FAMILY TREE (01 February 2021): https://www.facebook.com/jp.j.santiago/posts/10218211054244754
COVID MUTANTS: VARIANTS OF CONCERN (31 January 2021): https://www.facebook.com/jp.j.santiago/posts/10218204381877949
COVID MOLECULAR BIOLOGY: THE SPIKE (6 January 2021): https://www.facebook.com/jp.j.santiago/posts/10218019683340601