
COVID Variants Overview Update
COVID Variants Overview Update
Updated data from the 08 April version and the current variant trends in the United States

COVID VARIANTS OVERVIEW UPDATE
22 April 2021/Thursday/630pm PDT
“The variants are all the more reason to get vaccinated. The bottom line is the vaccines we are using very well protect against the dominant variant we have right now, and to varying degrees protect against serious disease among several of the other variants.”
-Anthony Fauci MD, 15 April 2021
High resolution version of today’s graphic: https://drive.google.com/.../1DLylXSpsZEoz5jAyM5I.../view...
BACKGROUND
My prior COVID table of the variants of concern and the variants of interest was done on 8 April and I posted it up on Facebook the following day. Many thanks to the physicians and scientists in my social media circles that have offered corrections, updates and reviews of the data as well as for continually educating me on the latest research. Today’s update is much like that one, only the table has been updated as yesterday, 21 April.
There are many news stories about COVID variants using terms like “double mutants” or something similar. Eric Topol MD, professor of molecular medicine at the Scripps Research Institute, once used the term “scariants” to refer to media coverage of the variants.
While such terms aren't completely accurate, the complexities of pandemic science don't lend themselves to quick sound bites and to some degree, perhaps such terminology is necessary to convey the seriousness at which the medical and scientific community view the rise of the variants.
The bottom line is that the vaccines available in the United States are still very effective, even against the new variants. We are losing momentum in our vaccination drive here in the United States and that is troubling given that the vaccines are our best defense against the variants combined with non-pharmacological interventions like public mask use, social distancing and capacity restrictions. The real world data from millions and millions of those vaccinated is highly encouraging and in the history of medicine, not just unprecedented in its scope as the largest mass vaccination campaign in history but also in its overall effectiveness and safety.
THE OVERVIEW TABLE
New items and data in the table compared to my previous version I posted to my Facebook page on 9 April (that table is dated 08 April in the upper left if you’re not sure what you have) are in blue text. I will run down each variant and touch on new information.
B.1.1.7
This more contagious and more lethal variant is now the dominant COVID variant in the United States, but it is still highly vulnerable to the antibodies that are elicited from vaccination. There are now 26 states where B.1.1.7 makes up more than 15% of the genomic surveillance samples with Tennessee, Colorado, Florida, and New Jersey most impacted in the last 60 days.
In the last 60 days, 36% of samples of the now over 300,000 samples from the United States in the GISAID genome database are B.1.1.7. In the UK, they are tracking a new sub-variant of B.1.1.7 that has the E484K mutation that dampens the immune response. Here in the United States, 64 samples of B.1.1.7 now have the E484K mutation and I expect that number to rise in the next several weeks.
While I have not seen the official listing of mutations in that Texas A&M student in the news lately, my suspicion based on statements made by public health officials so far is that the student was infected with B.1.1.7 with the E484K mutation. We’ll see once the genome data is available for review.
B.1.351
This variant does have the E484K mutation and one of the bumps in the AstraZeneca vaccine rollout in South Africa where B.1.351 emerged was that the vaccine wasn’t very effective against this variant. However, I should point out that the AstraZeneca vaccine candidate (which has not gotten its authorization for use in the United States yet) is still very effective against other variants like B.1.1.7.
B.1.351 has been found mostly in samples from South Carolina and North Carolina, constituting 2% of the samples from each of those states. While extensive in the states it’s been detected, its circulation continues to be a low levels. I hope it stays that way.
P.1
I updated when this variant likely emerged on the basis of my reading when I was creating that post on how surges can create variants. It’s date of emergence based on Nextstrain genetic data is sometime in the March to May 2020 time frame.
Data coming out of Brazil fits in with P.1 being twice as transmissible (contagious) as what we were dealing with before the arrival of B.1.1.7 in the United States. There is some question if it has a higher fatality rate- 1.2x to 1.9x higher, but there is some question if this is also a function of an overburdened health care system in Brazil. Before anyone makes that assumption that it’s the state of Brazil’s health care system, the data does show P.1 generates a higher viral load than what we have been dealing with before. The higher the viral load, the more vigorous the body’s inflammatory response which is part of the severity of COVID infection.
41 states have now detected P.1 and that’s up from before. The P.1 outbreak in British Columbia is very serious and remains the largest P.1 outbreak outside of Brazil, but there is a growing P.1 outbreak on Cape Cod in Massachusetts as well. The most P.1 found in the United States genome samples so far has been in Illinois where P.1 constitutes 4% of the samples in that state.
P.2
I also updated the likely date of emergence for P.2 to March to April 2020. This is also causing significant issues in Brazil and there is early data suggesting that mortality from P.2 infection is increased. There is a reduction in efficacy with the Johnson & Johnson vaccine with P.1 and given the similarities between P.1 and P.2, it’s possible we’ll see the same effect on that vaccine. But a reduction in efficacy does not mean resistance or the vaccine won’t work! Keep that in mind.
The genomic data suggests that P.2 diverged from a common ancestor with P.1 in April 2020 but it acquired the E484K mutation independent of P.1.
Remember, E484K dampens our immune response. So this is a very serious mutation and on my table, E484K is always in red to emphasize that point. In an upcoming post, I will be going into the molecular biology of E484K and why of all the mutations this one is the most significant.
For whatever reason, about 4% of the genomic samples coming from Maine are P.2.
B.1.427 AND B.1.429
Data shows a two-fold decrease in antibodies from the mRNA vaccines but they are still effective against these two variants because of our T-cells. Remember that our immune system has different arms- the humoral or antibody mediated immunity is from B-cells that produce antibody after being primed by vaccination. Cellular immunity is from the T-cells which directly target infected cells. It’s much easier to assess antibody levels than T-cell activity.
California, Nevada and Hawaii are the center of B.1.429 activity, but no state yet has reached 15% with B.1.427- however, it is 12% of samples in California, 10% in Nevada and 7% in Montana.
Both variants appear to induce viral loads twice as high as what we have dealt with before which is one of the mechanisms by which these two variants are more contagious.
B.1.525
This variant is still circulating at very low levels in the United States but has now been detected in 32 states. It is 19% of all samples in Nigeria but the state of testing in that nation has made a full assessment of its epidemiological impact challenging. This variant is 3% of samples in Rhode Island.
B.1.526
This is likely the second most worrisome variant in the United States after B.1.1.7, it’s increasing its spread in the US Northeast. More troubling is that it seems to have acquired the E484K mutation and the portion of B.1.526 samples with the E484K mutation has been increasing, it’s now at 77% of samples have the E484K mutation.
The epidemiological data out of New York is very suggestive that it’s more contagious. But despite the E484K mutation, early data is showing that the antibodies elicited from the mRNA vaccines are still effective.
This variant is now in 46 states with New York and New Jersey well over 15% prevalence in genomic samples in the last 60 days. New York alone is 28% which is very suggested of it being more transmissible.
B.1.526.1 AND B.1.526.2
These sub-lineages of B.1.526 has additional mutations and has been increasing as well, B.1.526.1 now 5% of all genomic samples in the state of New York. B.1.526.2 also continues its spread, it is 7% of samples in Rhode Island, 6% of samples in New York, and 5% of samples in New Jersey. They have both been detected in nearly all 50 states save 6 or 7 states.
B.1.617
This new variant of interest is not an official variant of interest with the CDC but I decided to add it as it is driving much of the severe surge going on in India right now. Hospitals throughout India are running out of medications, testing reagents for the laboratories, and most crucially oxygen supplies. They have put in requests for oxygen supplies through at least ten of their embassies in Western industrialized nations like the United States. My prior post covered B.1.617 in detail.
From my table, we can estimate from genomic data that B.1.617 likely emerged in March 2020 but was identified in October 2020. It’s key spike mutations are L452R (just like B.1.427 and B.1.429) but it has a variation of E484K designated E484Q. Based on the molecular biology of the mutations at position 484 on the spike, we suspect there will some reduction in the efficacy of vaccines and monoclonal antibody treatments, but not as significant as what we are seeing with E484K.
B.1.617 has been detected in 8 US states and is rapidly growing in prevalence in many of the provinces of India. Given the extensive trade, travel and IT sector links between the United States and India, this will be a variant we’ll need to keep a close eye on in the coming months.
VARIANT TRENDS IN THE UNITED STATES
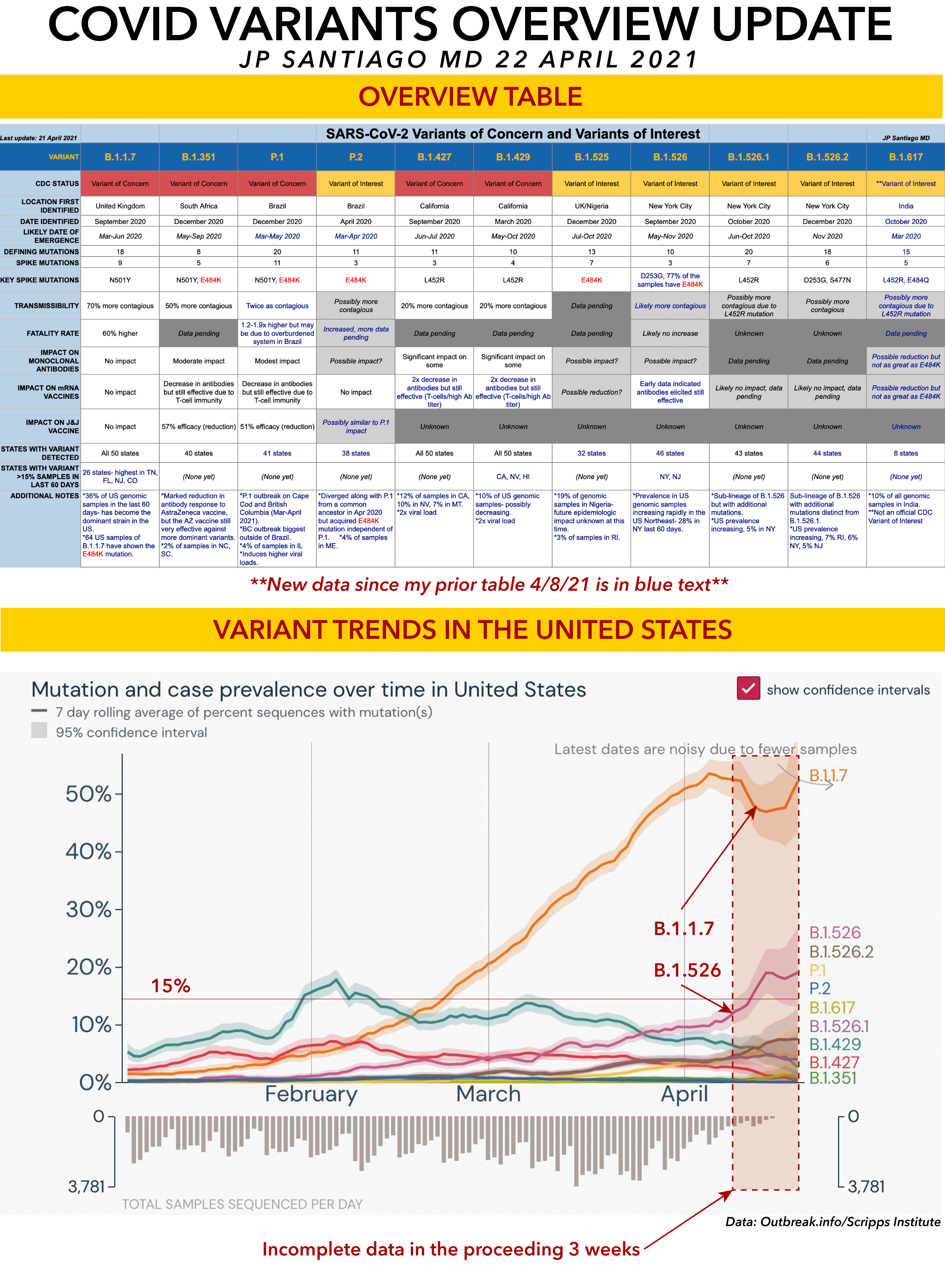
This graph of variant prevalence data comes from outbreak.info/Scripps Research Institute and I've set it to display all the variants except B.1.525 (it wasn't a selectable option) and their prevalence data in the United States from 1 January onward. Keep in mind that most of April's data is incomplete- note the lower graph showing the number of sequences uploaded to the GISAID genome database. There is still a lot of data from most of April that is still out there being processed.
As a rule of thumb, consider any prevalence data in this graph for the prior three weeks to likely be an undercount. Even if we accommodate for the possibility of an undercount, you can see that B.1.1.7 and B.1.526 are on the increase in this country.
The horizontal red line marks the 15% mark. That's an arbitrary point I use in my own data analysis routines that indicates that a given variant is likely spreading more widely than the prevalence data indicates.
TAKE HOME MESSAGES
1/ The genomic sequencing effort underway not just in the United States but worldwide will inevitably turn up further variants. That's a given.
2/ No variant has shown itself completely resistant to all of the available vaccines and those variants still under analysis have features at the genetic and molecular level that does not indicate we need to worry about the overall effectiveness of the available vaccines.
3/ As such, vaccination is still the best and most effective defense against ALL of these variants. The likely necessity of booster shots as early as this fall is to be better optimize our immune system defenses against these variants.
4/ There is no substitute for vaccination. Even a prior infection with COVID, regardless of how severe, does NOT generate a uniform, sustained, and optimized immune response like vaccinations can do.
5/ Variants possessing the E484K mutation are capable of dampening the immune response. B.1.526 has acquired this mutation and it is increasing within the pool of samples of B.1.526. It is likely also being picked up by B.1.1.7 as well. This is convergent evolution in action- multiple variant lineages independently gaining the E484K mutation.
6/ As I have emphasized in the past, each new infection is an opportunity to mutate for the virus. Limiting the number of new infections limits the number of chances the virus gets to mutate and try to gain the upper hand on our efforts.
PARTING THOUGHTS
Get your shot. Seriously. Many of us in medicine and science are tired already.
Exhausted and frustrated.
Sixteen months of this pandemic and we're still having to fight battles against misinformation, disinformation, toxic identity politics and privilege.
We can defeat this virus.
Can we defeat misinformation, disinformation, toxic identity politics and privilege?