
COVID VARIANTS UPDATE

30 June 2021/Wednesday/930pm CDT
"I do believe, in the United States at least, the potential for a very dramatic national surge is off the table because of the vaccination levels. ... [However,] unvaccinated people will continue to get infected, they will continue to get seriously ill, and they will continue to die."
-Michael Osterholm PhD/MPH, epidemiologist and director of CIDRAP (Center for Infectious Disease Research and Policy) at the University of Minnesota, 29 May 2021
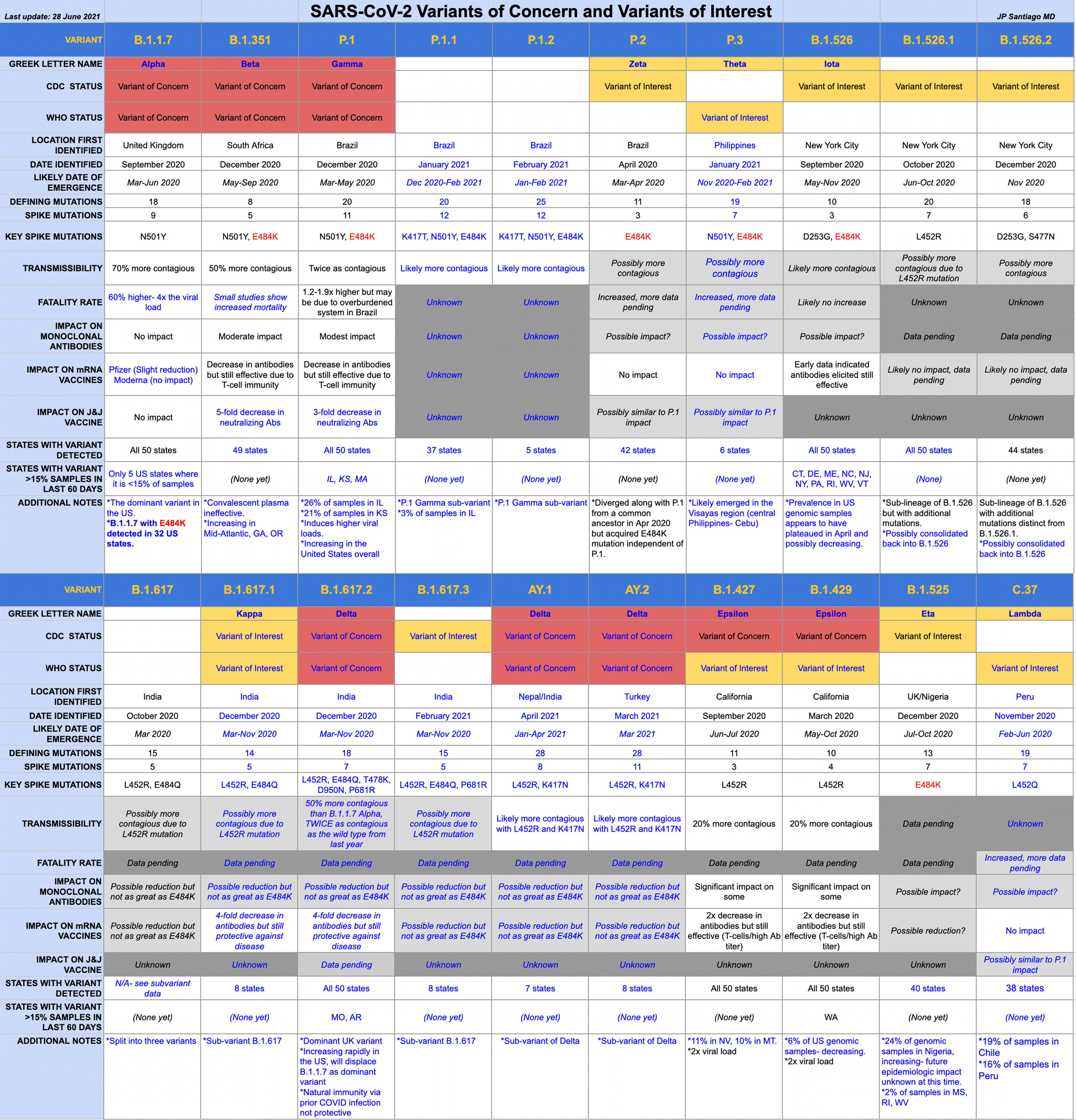
High resolution version of my latest version of the COVID Variants Table:
https://drive.google.com/file/d/1HGu56FIfSJ1xl6mOWBn4PCkgyj7HFMYC/view?usp=sharing
BACKGROUND
It's been a flurry of activity in the medical and scientific world since I released my prior version of the COVID Variants Table on May 22. As I have posted previously, case surges anywhere in the world increase the likelihood of the emergence of new variants. It's worth sharing again the quote from Dr. Thomas Friedrich, of the Department of Pathobiological Sciences, University of Wisconsin School of Veterinary Medicine:
“I think most people studying viral evolution agree that the appearance of these variants now mostly reflects the very large number of cumulative infections that have occurred worldwide since the start of the pandemic. On average, one mutation may occur every time or every other time the virus infects a new person. Each mutation is kind of like pulling a slot machine — the chance of hitting the jackpot on any individual pull is small, but you pull millions of handles simultaneously the chances are dramatically increased. Viruses that ‘hit the jackpot’ by accumulating a set of mutations that makes them more transmissible will then increase in the population due to natural selection."
Each new COVID infection is a chance for mutation- a surge need not be taking place. But a case surge offers thousands of opportunities each day for a mutation that can result in a new variant.
Since my prior release of the COVID Variant Table, the number of variants of significance has doubled in number. Part of that is on account of the fact that we're actively looking for variants now, but as cases surge in different parts of the world, new and increased opportunities for the emergence of new variants takes place.
VARIANT OF CONCERN VERSUS VARIANT OF INTEREST
There are three classifications of variants in order of increasing concern. Keep in mind that genomic surveillance as it continues to ramp up across the United States will find plenty of COVID variants. That's inevitable. Each time the virus infects someone new, that represents an opportunity to mutate and create a new variant. But not all variants are problematic. In fact, the majority of COVID variants we know about do not elicit the same level of concern that we have the variants I'll be talking about this evening.
Variant of Interest: "A variant with specific genetic markers that have been associated with changes to receptor binding, reduced neutralization by antibodies generated against previous infection or vaccination, reduced efficacy of treatments, potential diagnostic impact, or predicted increase in transmissibility or disease severity."
Variants of Interest (VOIs) have genetic mutations that *suggest* changes in how they are passed to others, how they might be diagnosed and treated, or how they might evade the immune system.
Variant of Concern: "A variant for which there is evidence of an increase in transmissibility, more severe disease (increased hospitalizations or deaths), significant reduction in neutralization by antibodies generated during previous infection or vaccination, reduced effectiveness of treatments or vaccines, or diagnostic detection failures."
Variants of Concern (VOCs) are *proven* to be more contagious, cause more serious disease and increase in mortality, and show increased resistance to medical therapies. They also possess mutations that can affect identification and diagnosis.
Variant of High Consequence: " A variant of high consequence has clear evidence that prevention measures or medical countermeasures (MCMs) have significantly reduced effectiveness relative to previously circulating variants."
Fortunately none of the variants have yet reached the level of "Variant of High Consequence". This is what Dr. Gregory Poland, one of the premier vaccine experts in the world, called "Variant X".
THINGS TO NOTE IN THIS RELEASE OF THE VARIANTS TABLE
1/ New information since the previous release is in blue text.
2/ I have added the Greek names for each of the variants where applicable.
3/ I have separated out which variants are VOCs and VOIs by either the CDC or the WHO.
4/ This is of course a dynamic situation as more research data is released and there may be sections in this table that are already in need of updating.
B.1.1.7 ALPHA
1/ Currently the dominant variant in the United States.
2/ Prevalence is starting to decline as B.1.617.2 Delta increases here in the US.
3/ Compared to the original virus we dealt with through most of last year, Alpha is much more contagious (70% more).
4/ Alpha also results in a 4x higher viral load in the body, resulting in not just in being more contagious but also more significant disease- about 60% higher fatality rate.
5/ The current vaccinations are effective against Alpha.
6/ Alpha is still the dominant variant in the US- while much is made about the dangers posed by B.1.617.2 Delta, if you are not vaccinated, Alpha is also still a very significant threat to you.
7/ There only 5 US states where Alpha is *NOT* greater than 15% of genomic surveillance samples.
8/ We are now seeing Alpha with the E484K mutation, that is a mutation of concern that provides for the ability to partially escape our immune response.
B.1.351 BETA
1/ Small studies are showing an increased death rate from B.1.351 Beta.
2/ While there are reductions in the neutralizing antibodies elicited from the vaccines when it comes to B.1.351 Beta, one of the other arms of the immune system, the T-cells helps offset this reduction.
3/ Convalescent plasma is ineffective against Beta.
4/ While not increasing in the US as fast as B.1.617.2 Delta, Beta is growing in prevalence in Georgia, the Carolinas, Virginia and Oregon.
5/ If you are not vaccinated, Beta is a threat to you.
P.1 GAMMA
1/ Now present in all 50 states, P.1. Gamma is the second fastest growing variant in the United States after B.1.617.2 Delta.
2/ P.1 Gamma is about twice as contagious as the virus we dealt with through most of last year.
3/ The current vaccines are effective against Gamma despite reductions in elicited antibodies.
4/ If you are not vaccinated, Gamma thanks to the E484K mutation is a significant threat to you.
P.1.1 AND P.1.2
1/ P.1 Gamma sub-variants that emerged in Brazil in the first quarter of this year during their surge.
2/ Not a VOI or VOC yet with either the CDC or the WHO, these sub-variants are worth watching as they possess the K417T mutation which may increase their contagiousness.
P.2 ZETA
1/ Not as big of an issue in the United States right now but considered a VOI by the CDC.
P.3 THETA
1/ This variant is related to P.1 and P.2 and emerged in the central Philippines in the first quarter of this year.
2/ The WHO has classified Theta as a VOI as it has similarities to P.1 and P.2
B.1.526 IOTA AND ITS SUBVARIANTS
1/ Eight weeks ago I was concerned about the rise in Iota in the US Northeast but its prevalence appears to be decreasing.
2/ I am not entirely sure but the B.1.526.1 and B.1.526.2 sub-variants may have been rolled back into the B.1.526 parent variant for classification purposes. Like the Iota parent variant, these sub-variants have also been on an overall decrease in the United States.
B.1.617
1/ This is the parent variant for both B.1.617.1 Kappa and the better known B.1.617.2 Delta.
B.1.617.1 KAPPA AND B.1.617.3
1/ Two of the 617 sub-variants, right now this variant is more of an issue in India but has been detected in 8 US states.
2/ B.1.617.3 may be less contagious than Kappa. The CDC classifies both as Variants of Interest.
3/ The mRNA vaccines are protective still against Kappa.
4/ While it is circulating in possibly low levels in the US, this variant is as much a threat to the unvaccinated as the other variants.
B.1.617.2 DELTA
1/ This will become the dominant US variant before the end of the summer if not sooner. It is already the dominant variant in some US locations (like Missouri).
2/ Delta is considered a VOC by both the CDC and the WHO.
3/ Delta is 50% more contagious than B.1.1.7 Alpha and twice as contagious as the virus we dealt with through most of last year.
4/ Delta possess point mutations in its spike protein that makes it highly efficient at infecting unvaccinated individuals.
5/ This variant is now present in all 50 US states and increasing exponentially, particularly among the unvaccinated.
6/ Vaccines are still protective against Delta despite reductions in the elicited antibodies. Keep in mind that antibodies are not the only weapon in the immune system's armory but a very easy biomarker to assess.
7/ Natural immunity from prior COVID infection will not protect you against infection with Delta.
AY.1 DELTA AND AY.2 DELTA
1/ AY.1 is the Delta subvariant is sometimes called "Delta Plus" in some news stories.
2/ AY.1 and AY.2 are very similar to each other and both variants are considered VOCs by both the CDC and WHO.
3/ Both of these Delta sub-variants likely emerged in the spring of this year.
4/ Potential combination of L452R and K417N mutations in the same variant has us concerned this may make these Delta sub-variants more contagious than Delta itself.
B.1.427/B.1.429 EPSILON
1/ These are the variants that emerged in California last year and likely had a hand in the holiday surges in that state.
2/ Overall prevalence in the United States is decreasing but still a threat on the US West.
B.1.525 ETA
1/ Eta continues to increase in the samples from West Africa.
2/ Eta has been detected in 40 US states but at low levels.
C.37 LAMBDA
1/ Lambda likely emerged in Peru at the end of last year and has only recently been characterized.
2/ The L452Q mutation is new to me, so I'm not sure how it will affect this variant's behavior compared to L452R that we know more about thanks to that mutation being more widespread across several variants.
3/ C.37 Lambda is increasing on the west coast of South America- mostly Chile and Peru right now, but it has been detected in 38 US states.
TAKE HOME MESSAGES
1/ Data so far indicates that vaccination is still the best defense against all of these variants.
2/ While there are decreases in neutralizing antibodies elicited by vaccination with some of these variants, overall protection against hospitalization and death from COVID is still robust.
3/ Many of these variants, however, may likely reduce the ability of the vaccines to stop asymptomatic infection and mild disease. There is a significant difference between stopping transmission of COVID and preventing COVID death and hospitalization.
4/ If you are unvaccinated despite being eligible for vaccination, many of these variants are a clear and present danger to you to a degree that we did not see in this pandemic last year.
5/ It is likely we will see more breakthrough infections amongst the vaccinated with these variants- but those infections are likely to be mild.
6/ A more contagious variant means not only is public mask use necessary but special attention must be paid to the pediatric population too young for vaccination. These variants are going to challenge many of the assumptions we have about COVID in children. Any variant that is more efficient at infection constitutes a special threat to our children who are not able to get vaccinated yet.
PARTING THOUGHTS
2021 is shaping up to not just be a race between vaccinations and variants but it is also a tale of two different pandemics- those who are vaccinated versus those who are not vaccinated. Hospitalizations and deaths in the United States are now occurring nearly exclusively among the unvaccinated.
Those who are vaccinated can still get infected and can still develop symptomatic COVID. But not to the same degree as those who are unvaccinated.
Many of us are anticipating issues with the coming increase in the prevalence of the Delta variant- not just among the unvaccinated but also among our children who are too young for vaccination. Much of what we have come to learn about pediatric COVID in 2020 may need to be rewritten and updated this fall when school starts.
Assumptions and understanding are going to be challenged in new ways in the next six months.
RELEVANT PAST POSTS (Facebook links)
MAYO CLINIC GRAND ROUNDS: VACCINES AND VARIANTS (14 June 2021): https://www.facebook.com/jp.j.santiago/posts/10219031846404045
THE MOLECULAR BIOLOGY OF THE E484K MUTATION (10 May 2021): https://www.facebook.com/jp.j.santiago/posts/10218832046529173
IMMUNOLOGY 101: THE IMMUNE SYSTEM- REPOST/UPDATE (05 May 2021): https://www.facebook.com/jp.j.santiago/posts/10218801066954703
COVID VARIANTS OVERVIEW AND UPDATE (22 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218722676514991
NEW COVID VARIANT OF INTEREST: B.1.617 (18 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218699298170547
CASE SURGES CAN RESULT IN COVID VARIANTS (12 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218657527966318
THE OVERVIEW & STATUS OF COVID VARIANTS (9 April 2021): https://www.facebook.com/jp.j.santiago/posts/10218637120816152
QUICK UPDATE: THE COVID FAMILY TREE (01 February 2021): https://www.facebook.com/jp.j.santiago/posts/10218211054244754
COVID MUTANTS: VARIANTS OF CONCERN (31 January 2021): https://www.facebook.com/jp.j.santiago/posts/10218204381877949
COVID MOLECULAR BIOLOGY: THE SPIKE (6 January 2021): https://www.facebook.com/jp.j.santiago/posts/10218019683340601